The Impact of Language Deprivation on the Overall Development of Deaf and Hard of Hearing Children
“Communication Access” Lauralee, age 6
For decades psychologists, medical professionals, and researchers have known that there is a critical period for language acquisition in humans. That critical period is approximately the first 5 years of a child’s life when there is an elevated neurological sensitivity for language development (Hall et al, 2017; Gulati, S. 2014).
Language deprivation during the critical period appears to have permanent consequences for long-term neurological development.
Language deprivation occurs due to a chronic lack of full access to a natural language during that critical period. For Deaf and Hard of Hearing students, parents and professionals must understand that access to language and language development is a crucial part of the of the overall functioning of children and adolescents. In fact, I might argue, that understanding its impact is the central issue that school and clinical psychologists must understand in order to conduct ethical and effective evaluations of cognitive, academic and social-emotional functioning. But instead of “nerding” out about the diagnostic process, let me instead explain language deprivation and what it looks like in the growing Deaf or Hard of Hearing child, talk about the ways in which language deprivation can impact the growing child, the grown adult, and whether or not hearing levels dictate the significance of language deprivation impact. This article will be heavily ladened with research references for a few reasons: 1) I hope you can use this for your own resource when you are discussing this issue with others. 2) I want you, the reader, to understand that my position is based not only on my 20+ years of experience assessing Deaf and Hard of Hearing children, but also on years of research in this field. My colleagues in this field have conducted many rich, valid studies that have helped to elucidate the field and provide the foundation for my work. Oh and 3) I’m a nerd. I mentioned that, right? I love research and numbers.
What is language deprivation?
As I mentioned above, language deprivation occurs due to a chronic lack of full access to a natural language during the critical period of a child’s life, the first five years where neuroplasticity is at its peak. First, let’s define “natural language.” By this I am referring to any spoken or signed language such as that accepted and generally used by the community / country within which the child lives. For the purposes of this article, this will mean spoken English (even when the home language may be Spanish*) and American Sign Language (ASL). ASL is distinguished from artificial, though helpful, communication systems such as Cued Speech, which can be used as a tool to help develop English skills. Natural language is also distinguished from the Listening and Spoken Language approach (LSL), which is historically known as oralism. LSL is, itself, not a language. It is a systematic approach to teaching English to Deaf children in the US (or other spoken languages in their country of origin).
Despite ample research to show that ASL is a formal language with its own grammar and linguistic rules, less than 8% of Deaf children receive regular access to sign language in the home (Liddel, SK, 2003; Institute, G.R., 2011). Although using ASL is encouraged for hearing babies to develop language skills before they can begin to speak, ASL is not routinely offered as a primary or complementary intervention for Deaf children; rather, if offered at all, it is often proposed as a last-resort option to Deaf children who have not developed speech abilities as expected (Humphries, T. et al 2012). This pattern occurs because many advocates, professionals, and educators believe that ASL acquisition will interfere with a Deaf child’s development of speech skills (Lyness, C. et al 2013; Sugar, M. 2016; Davidson, et al 2011; Duchesne et al. 2009; Lund 2015; Tobey at al, 2011) despite research showing that children with cochlear implants who use ASL actually demonstrate better speech skills, language development and intelligence scores than non-signing children (Davidson, et all 2011; Hassanzadeh, S. 2012; Amraeri, K. 2016). Based on current research, technological intervention alone (i.e., hearing aids, cochlear implants) are insufficient as a stand-alone approach for language acquisition in Deaf children (Humphries et al 2012b; Kral et al 2016). The research is showing us that hearing aids and cochlear implants, when used alone (i.e., without the support of ASL) do not give sufficient access to language to prevent language deprivation in Deaf and Hard of Hearing children.
What does this mean? The truth is, if a Deaf child or Hard of Hearing child does not have access to ASL they are likely experiencing some level of language deprivation. Yup, I said it. I am not saying ASL only, ASL instead of, ASL at the exclusion of speech. I actually believe that children should have options and parents should take advantage of the tools that the medical field offers them. But the research has spoken and it is strong: Hearing aids or cochlear implants alone do not provide adequate access to language and should be used in conjunction with ASL.
How significant is the impact?
For decades clinicians have observed that children who suffered from language deprivation during the critical period have a unique presentation. We noted that the language of many Deaf and Hard of Hearing children seemed delayed, more concrete, and lacking in fundamental components despite attempts to intervene. More recent neuroimaging studies have finally clarified the reason. Language deprivation during the critical period appears to have permanent consequences for long-term neurological development (Leybert, J. & D’Hondt, M., 2003). So much so, that specific timing and quality of language access during early childhood can cause neurostructural differences (Mayberry et al, 2011; Penicaud, et al 2013; Skotara, et al, 2012).
Language dysfluency and child presentation
Languages (auditory or visual) have rules and structures that make them languages; language dysfluency is a disruption of these rules and structures. In Deaf children with dysfluency this may look like limited vocabulary, lack of time markers (i.e., days, weeks, month, year), inaccurate spatial organization (a grammatical construct), and a lack of syntax; vocabulary may be more “concrete” and limited to actions and descriptions the child / adolescent has experienced directly (Glickman, N.S. 2007).
These children, and later adults, also demonstrate comprehensive knowledge deficits which are best described as gaps in knowledge due to an accumulate lack of environmental information or incidental learning (Schenkel, L.S. et al 2014). Understand that normal acquisition of passive information is made through media, radio, newspapers, TV, and word of mouth – avenues typically not easily accessible to Deaf and Hard of Hearing individuals. However, current social media, the internet and captioned TV makes it easier if Deaf and Hard of Hearing individuals have the vocabulary to access these resources and the communication accessibility at home to discuss these resources with their family members. When family members do not know ASL, the captioning is not turned on on TVs around the house, the internet is not captioned, newspapers or magazines are not available (and age appropriate), Deaf and Hard of Hearing children only have access to incidental learning during the 4 to 8 hours they are in a signing environment within the classroom (assuming they are placed with signing peers). The consistent lack of exposure to everyday opportunities results in an overall loss of understanding of many aspects of societal functioning, such as school interactions (when they are not in a larger program with Deaf peers), government functions, personal behaviors, etc. This can have a long term impact on a Deaf child’s physical, mental and social health.
What areas of functioning are impacted?
There does not appear to be any evidence that language cannot be learned through multiple modalities (i.e. through a combination of ASL and the use of hearing aids or cochlear implants). Nor does there appear to be any evidence that using ASL impairs spoken language development, but there is strong evidence that a lack of language access will cause long term negative consequences (Lederberg et al 2013). The risk for secondary or tertiary diagnoses in Deaf or Hard of Hearing individuals seems more magnified due to language deprivation. There is evidence that language deprivation can cause cognitive delays (Niparko, J.K. et al 2010; Davidson, L.S., 2011; Tobey, E.A., et al 2011; Lund, E. 2015). Deaf and Hard of Hearing children who have a history of language deprivation are also more likely to experience abuse, trauma or exploitation (Pollard 2014; Schenkel et al, 2014). In addition, there are also studies that demonstration that Deaf and Hard of Hearing children who have suffered language deprivation also have much higher incidences of behavioral disorders (Stevenson, J. et al 2010; Barker, D.H., et al 2009). Furthermore, language deprivation leads to the inability to develop “theory of mind” (the idea that other people think differently than you do) (Ketelaar, Rieffe, Wiefferink, & Frijns, 2012). Finally, the failure to develop adequate language skills may be associated with failures to develop empathic attunement (empathy) with other people (Gulati, 2019).
Dr. Neil Glickman described the impact of language deprivation quite well in his introduction for a Webinar (2018): “The mental health skills we refer to as emotional self-regulation, or coping, which is the focus of so much contemporary cognitive behavioral therapy, can be done without language (think of sensory strategies like rocking or jumping for self-regulation). However, understanding the concept of self-regulation and advancing beyond sensory movement interventions, requires formal language. Certainly, language deprivation can dramatically limit one’s set of strategies for self-regulation.” Glickman goes on to note that interpersonal skills such as communication, problem-solving, and conflict resolution, which are also common foci of evidenced-based Cognitive Behavioral Therapy (CBT), require formal language (Glickman, 2009, 2017).
As mentioned above, language deprivation can have long term consequences on cognitive skills. I can share from my professional experience that I see a consistent impact on Verbal IQ as measured by the Wechsler Intelligence Tests. These happen to be my favorite intelligence tests because they have adapted well over the years, they give directions for use with Deaf and Hard of Hearing students and they include a small number of Deaf kids in their norming samples now. Of course there are other very good tests but I won’t go off on that tangent. Back to Verbal IQ. Intelligence, generally speaking, is the ability to problem solve and come up with new solutions given a new problem. Easy, right? Not so much. Problem solving, really good problem solving, requires language, organization skills, high level thinking skills, the incorporation of past knowledge and experiences, and the ability to develop and test hypotheses in one’s mind before they come to fruition. I could go on. Intelligence is not just one construct – language or spatial skills, but many different constructs.
Why am I explaining all this? First, because too often I see other psychologists (that do not frequently work with Deaf or Hard of Hearing students) ignore Verbal skills in Deaf children or, even worse, assume they are “nonverbal” if they do not speak (verbal means language not just spoken language). Second, because verbal skills are most closely linked to academic success. It is important to assess verbal skills of Deaf and Hard of Hearing children if we are to get an idea of what is impacting their academic progress. What I have seen time and again is that Deaf and Hard of Hearing children who have suffered from language deprivation during the critical early years often have lower Verbal IQ scores later. Frequently, I will see Deaf and Hard of Hearing children with Average Nonverbal IQ scores but Extremely Low Verbal IQ scores. I have noticed that when sign language intervention is provided later (after age 5), Verbal IQ scores do improve but never up to the same level as the Nonverbal IQ. As such, in my experience, the effect of early language deprivation is permanent. Unfortunately, the most negative impact is on Verbal IQ which is most highly correlated with academic functioning.
Over the course of my career I have had the honor of assessing or supervised the assessment of thousands of Deaf and Hard of Hearing children. I have observed that speech skills are not the same as having good language skills. What does this mean? I have seen many Deaf and Hard of Hearing children, raised without ASL during the first 5 years, who have intelligible speech and can carry on a conversation with a hearing person without the use of ASL. However, when I actually test their Verbal IQ, I find the same profile that I do of any child with a history of language deprivation. Many of these children can talk but speech is not language. This is an important concept to understand. Speech is not language. Speech is important but it is one component of language. Language skills are so much more complex. The most important single feature characterizing human language is its infinite productivity and creativity (i.e. ability to problem solve new problems). Human beings are unrestricted in what they can communicate; no area of experience is accepted as necessarily incommunicable, even when we discover new things or new modes of thought. Having intelligible speaking skills does not, however, mean having adequate language skills.
 Is there a difference in impact based on hearing levels?
Is there a difference in impact based on hearing levels?
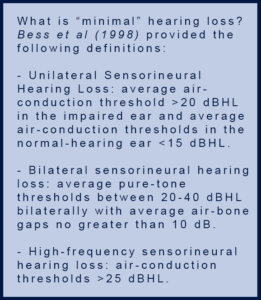
All too often I hear from parents whose children are not getting support from their school districts because the staff psychologist or audiologist or speech teacher has reported that the hearing loss is not “significant enough” to require intervention (i.e. a 504 plan or an IEP delineating special services such as a FM system, speech services, Resource Specialist Program (RSP), services by a Deaf and Hard of Hearing (DHH) itinerant teacher, placement in a Deaf program, etc.). It is my opinion, that most hearing loss warrants intervention and support. Research shows that even “minimal” hearing loss can have an impact on the educational access of a child.
This degree of hearing loss has also been described as “subtle,” “slight,” and “mild.” However, the use of these terms belies the fact that many individuals with these degrees of hearing loss exhibit more than minimal difficulties as a result. On this issue I can speak from experience. Over the last 10-15 years I have slowly lost my mid-range hearing (of those consonants in the speech banana). I still have a “mild” hearing loss, but some days it does not feel mild. In a one-to-one setting, I do just fine. But put me in a crowd or in a large space (like a classroom or gym or restaurant) and I get lost quickly. I experience ringing in my ears or I am tired or I don’t feel like putting in the extra effort to discriminate the words of the people talking around me. It is a day to day adventure because sometimes I am fine and other days I would rather not bother.
 As early as 1980, research started to emerge that indicated that as many as a third of children with unilateral hearing loss (UHL) failed at least one grade in school and 50% either failed a grade or required additional resources (Humes, L.E. et al 1980; Bess, F.H. & Tharpe, A.M., 1986; Bess, F.H. et al 1986; Culbertson, J.L. & Gilbert, L.E., 1986; Klee T.M. & Davis-Dansky, E.A., 1986; Bess, F.H. & Tharpe, A.M., 1984; Oyler, R.F. et a; 1988; Bovo, R. et al 1988; Hartvig Jensen J, et al 1989; Watier-Launey C. et al 1998). Another important research finding was discovered by Bess and her colleagues. They found that despite the long-held belief that children with UHL would have little difficulty listening as long as speech was directed toward their hearing ear (monaural direct with speech directed toward the normal-hearing ear and noise directed to the poor ear), Bess et al demonstrated that in quiet or with background noise, children with UHL had poorer speech perception scores than their normal hearing peers regardless of the location of the speech signal source (Bess, F.H. & Tharpe, A.M., 1986). Interestingly, research has not shown specific deficits with speech and language abilities of children with UHL versus hearing peers. However, research has shown lower verbal IQ scores in children with UHL (Klee T.M. & Davis-Dansky, E.A., 1986).
As early as 1980, research started to emerge that indicated that as many as a third of children with unilateral hearing loss (UHL) failed at least one grade in school and 50% either failed a grade or required additional resources (Humes, L.E. et al 1980; Bess, F.H. & Tharpe, A.M., 1986; Bess, F.H. et al 1986; Culbertson, J.L. & Gilbert, L.E., 1986; Klee T.M. & Davis-Dansky, E.A., 1986; Bess, F.H. & Tharpe, A.M., 1984; Oyler, R.F. et a; 1988; Bovo, R. et al 1988; Hartvig Jensen J, et al 1989; Watier-Launey C. et al 1998). Another important research finding was discovered by Bess and her colleagues. They found that despite the long-held belief that children with UHL would have little difficulty listening as long as speech was directed toward their hearing ear (monaural direct with speech directed toward the normal-hearing ear and noise directed to the poor ear), Bess et al demonstrated that in quiet or with background noise, children with UHL had poorer speech perception scores than their normal hearing peers regardless of the location of the speech signal source (Bess, F.H. & Tharpe, A.M., 1986). Interestingly, research has not shown specific deficits with speech and language abilities of children with UHL versus hearing peers. However, research has shown lower verbal IQ scores in children with UHL (Klee T.M. & Davis-Dansky, E.A., 1986).
Environmental factors also impact the Hard of Hearing child in the classroom. The acoustic set up in the classroom has a significant impact on speech perception and learning in children and ultimately can have a negative impact on academic progress. Multiple studies have assessed the poor acoustics in the typical classroom (Bess, F.H. et al 1984; Knecht H.A, et al 2002; McCroskey, &F., Devens, J. 1975; Picard, M. & Bradley, J. 2001) as well as the adverse effects noise can have on the learning of children with hearing loss (Boney S. & Bess, F. 1984; Crandell, C.C. 1993; Finitzo-Hieber, T. & Tillman T. 1978; Hawkins D.B. & Yacullo, W. 1984). Typical accommodations in the classroom are seating in the front of the classroom, but does the teacher (and student) also remember to look for noise making items like the air conditioning unit, the door to the classroom, the tapping from a student’s pencil or kids talking, the cabinets or desk tops that open and close? Even when the teacher is using a FM system (assuming the teacher and student are compliant with its use), these noise makers can negatively impact the effectiveness of amplification. For the Hard of Hearing child, working all day to filter out these sounds can result in cognitive fatigue. Cognitive fatigue is simply that tiredness or fatigue that sets in after working on mentally tasking activities for long periods of time. Hard of Hearing and Deaf children using hearing aids (HAs) or cochlear implants (CIs) do not have predictable access to sound so the brain can not really habituate to noise. This means the brain is working harder all day to filter out noise and understand what is being said. This does not even take into consideration the noise variations that occur over the course of the day – from the classroom, the playground, the gymnasium, the cafeteria. All of these areas have different acoustic characteristics and staff members may not all have experience successfully using the FM system. If a child is coming home exhausted after school or is complaining about feeling too tired or is having difficulty focusing on lessons in the afternoon, it could just be from the effort involved in trying to attend to the teacher’s lecture all day, while filtering out noise.
No matter the hearing loss, the impact is experienced by the person with the hearing loss. They are the narrators of their own story and their experience needs to be understood in its entirety. As professionals and parents, we have an obligation to provide for our children all of the options needed to access their education. Deaf education has historically been tarnished by the arguments between the “oralists” and the “manualists”. The fact is, Deaf and Hard of Hearing children need access to their natural language of ASL and their parents have the right to utilize whatever medical tools are at their disposal to give their child more opportunities. Deaf children have the right to grow up bilingual – in ASL and English (spoken and / or written). Hearing aids and cochlear implants (and whatever new medical technology that comes along) need to be recognized for what they are – tools.
Conclusion
Is language deprivation real? Yes. Does it impact the majority of Deaf and Hard of Hearing children? I would venture to say yes, if they have not had access to ASL at school and home from birth. Do hearing aids and cochlear implants prevent language deprivation? When used alone, no. Access to ASL is needed. Access to visual information is needed. The child’s need for ASL instruction should be assessed by a qualified team of professionals. Special attention needs to be given to making sure the classroom is also acoustically accessible if the child is using HAs or CIs.
Language deprivation is preventable. We adults need to prevent it. We can do better by Deaf and Hard of Hearing children and we should (Hall, 2017).
 M. Natasha Kordus, Ph.D. Dr. Kordus received her Ph.D. from Gallaudet University in Washington DC in 1998. She has since worked at the California School for the Deaf in Fremont, St. John’s Mental Health Center in Santa Monica and the California School for the Deaf in Riverside. Dr. Kordus is a licensed Clinical Psychologist, credentialed School Psychologist and Behavior Specialist. She has her Pupil Personnel Credential in School Psychology and a Clear Credential in Administration. For the past 9 years she has supervised the Assessment Services and the California Deaf Education Resource Center at the California School for the Deaf in Riverside. She is fluent in ASL.
M. Natasha Kordus, Ph.D. Dr. Kordus received her Ph.D. from Gallaudet University in Washington DC in 1998. She has since worked at the California School for the Deaf in Fremont, St. John’s Mental Health Center in Santa Monica and the California School for the Deaf in Riverside. Dr. Kordus is a licensed Clinical Psychologist, credentialed School Psychologist and Behavior Specialist. She has her Pupil Personnel Credential in School Psychology and a Clear Credential in Administration. For the past 9 years she has supervised the Assessment Services and the California Deaf Education Resource Center at the California School for the Deaf in Riverside. She is fluent in ASL.
*Note from the author: I am a firm believer that children with true access to multiple languages can learn them all. For Deaf and Hard of Hearing children in the United States, their access to Spanish at home varies significantly. For many of the same reasons that hearing aids (HAs) alone cannot give full access to spoken English, they cannot give access to spoken Spanish without direct instruction / intervention. Direct Spanish instruction is not provided in most American schools therefore, the primary challenge is to get our kids first fluent in, ideally, ASL and English.
References:
Humes, L.E., Allen, S.K. & Bess, F.H. (1980) Horizontal sound localization skills of unilaterally hearing-impaired children. Audiology; 19: 508-518.
Bess, F.H. & Tharpe, A.M. (1986). Case history data on unilaterally hearing-impaired children. Ear Hear; 7:14-19.
Bess, F.H., Tharpe, A.M., & Gibler, A.M. (1986). Auditory performance of children with unilateral hearing loss. Ear Hear; 7:20-26.
Culbertson, J.L. & Gilbert, L.E. (1986). Children with unilateral sensorineural hearing loss. Ear Hear; 7(1): 38-42.
Klee T.M. & Davis-Dansky, E.A. (1986). A comparison of unilaterally hearing-impaired children and normal-hearing children on a battery of standardized language tests. Ear Hear; 7(1):27-37.
Bess, F.H. & Tharpe, A.M. (1984). Unilateral hearing-impairment in children. Pediatrics; 74(2):206-216.
Oyler, R.F., Oyler, A.L., & Matkin, N.D. (1988). Unilateral hearing loss: demographics and educational impact. Language Speech Hearing Services in Schools; 19:201-210.
Bovo, R., Martini, A., Agnoletto, M, et al (1988). Auditory and academic performance of children with unilateral hearing loss. Scandinavian Auditory Supplementum: 30:71-74
Hartvig Jensen J, Borre S., & Johansen, P.A. (1989). Unilateral sensorineural hearing loss in children: cognitive abilities with respect to right / left differences. British Journal of Audiology; 23:215-220.
Watier-Launey C., Soin, C., Manceau, A., & Ployet, M.J. (1998). Necessity of auditory and academic supervision in patients with unilateral hearing disorder: retrospective study of 175 children. Ann Otolaryngol Chir Cervicofac; 115:149-155.
Hall, W., Levin, L.L. & Anderson, M.L. (Febuary, 2017). Language deprivation syndrome: a possible neurodevelopmental disorder with sociocultural origins. Social Psychiatry and Psychiatric Epidemiology.
Liddel SK (2003) Grammar, gesture, and meaning in American Sign Language. Cambridge University Press, New York, NY
Institute GR (2011) Regional and national summary report of data from the 2009-10 annual survey of deaf and hard of hearing children and youth. pp 1-12
Humphries T, Kushalnager P, Mathur G, Napoli DJ, Padden C, Rathmann C, Smith SR (2012) Language acquisition for deaf children: reducing the harms of zero tolerance to the use of alternative approaches. Harm Reduct J 9:16. doi:10.1186/1477-7517-9-16.
Lyness C, Woll B, Campbell R, Cardin V (2013) How does visual language affect crossmodal plasticity and cochlear implant success? Neurosci Biobehav Rev 37:2621-2630.
Sugar M (2016) Dispelling myths about deafness. https://web.archive.org/web/20160404050959/http://www.agbell.org/in-the-news/response-nyle-dimarco/?. Accessed 4 Apr 2016
Hassanzadeh S (2012) Outcomes of cochlear implantation in deaf children of deaf parents: comparative study. Journal of Laryngology and Otology 126(10):989-994. doi:10.1017/S0022215112001909
Amraei K, Amirsalari S, Ajallouiyan M (2016) Comparison of intelligence quotients of first- and second-generation deaf children with cochlear implants. International Journal of Pediatric Otorhinolaryngol 92:167-170. doi:10.1016/j.ijporl.2016.10.005
Humphries T, Kushalnagar P, Mathur G, Napoli DJ, Padden C, Rathmann C, Smith SR (2016) Avoiding linguistic neglect of deaf children. Social Services Review 90(4):589-619. doi:10.1086/689543
Kral A, Kronenberger WG, Pisoni DB, O’Donoghue GM (2016) Neurocognitive factors in sensory restoration of early deafness: a connectome model. Lancet Neurology 15(6):610-621.doi:10.1016/S1474-4422(16)00034-X
Leybaert J, D’Hondt M (2003) Neurolinguistic development in deaf children: the effect of early language experience. International Journal of Audiology 42(Suppl 1):S34-S40
Mayberry RI, Chen JK, Witcher P. Klein D (2011) Age of acquisition effects on the functional organization of language in the adult brain. Brain and Language 119(1):16-29. Doi:10.1016/j.bandl.2011.05.007
Penicaud S. Klein D, Zatorre RJ, Chen JK, Witcher P, Hyde K. Mayberry RI (2013) Structural brain changes linked to delayed first language acquisition in congenitally deaf individuals. Neuroimage 66:42-49. Doi:10.1016j.neuroimage.2012.09.076
Skotara N, Salden U, Kugow M, Hanel-Faulhaber B, Roder B (2012) The influence of language deprivation in early childhood on L2 processing: an ERP comparison of deaf native signers and deaf signers with a delayed language acquisition. BMC Neuroscience 13:44, doi:10.1186/1471-2202-13-44
Glickman NS (2007) Do you hear voices? Problems in assessment of mental status in deaf persons with severe language deprivation. Journal of Deaf Studies and Deaf Education 12(2):127-147. doi:10.1093/deafed/enm001
Schenkel LS, Rothman-Marshall G, Schlehofer DA, Towne TL, Burnash DL, Priddy BM (2014) Child maltreatment and trauma exposure of deaf and hard of hearing young adults. Child Abuse Neglect 38(10):1581-1589. doi:10.1016/j.chiabu.2014.04.010
Lederberg AR, Schick B, Spencer PE (2013) Language and literacy development of deaf and hard of hearing children: successes and challenges. Developmental Psychology 49(1):15-30. Doi:10.1037/a0029558
Davidson LS, Geers AE, Blamey PJ, Tobey EA, Brenner CA (2011) Factors contributing to speech perception scores in long-term pediatric cochlear implant users. Ear Hear 32(1 Suppl):19S-26S. doi:10.1097/AUD.0b013c3181ffdb8b
Bess, F.H., Sinclair, S. & Riggs, D. (1984). Group amplification in schools for the hearing-impaired. Ear Hear; 5: 138-144.
Knecht H.A, Nelson, P. Whitelaw, G., & Feth, L. (2002). Background noise levels and reverberation times in unoccupied classrooms: predictions and measurements. American Journal of Audiology; 11:65-71.
McCroskey, & F., Devens, J. (1975). Acoustic characteristics of public school classrooms constructed between 1890 and 1960. NOISEXPO Proceedings: 101-103.
Picard, M. & Bradley, J. (2001). Revisiting speech interference in classrooms. Audiology; 40: 221-244.
Boney S. & Bess, F. (November, 1984). Noise and reverberation effects in minimal unilateral sensorineural hearing loss. Paper presented at American Speech-Language-Hearing Association annual convention; San Francisco, CA.
Crandell, C.C. (1993). Speech recognition in noise by children with minimal degree of sensorineural hearing loss. Ear Hear; 14: 210-216.
Finitzo-Hieber, T. & Tillman T. (1978). Room acoustics effects on monosyllabic word discrimination ability for normal-hearing and hearing-impaired children. Journal of Speech and Hearing Research; 21:440-458.
Hawkins D.B. & Yacullo, W. (1984). Signal-to-noise ratio advantage of binaural hearing aids and directional microphones under different levels of reverberation. Journal of Speech and Hearing Disorders; 49:409-418.
Glickman, N. (2018) Language Deprivation and Deaf Mental Health: Introduction to the Webinar
Ketelaar, L., Rieffe, Wiefferink, C., & Frijns, J. H. N. (2012). Does hearing lead to understanding? Theory of mind in toddlers and preschoolers with cochlear implants. Journal of Pediatric Psychology, 37(9), 1041–1050.
Gulati, S. (2019). Language deprivation syndrome. In N. Glickman & W. Hall (Eds.), Language deprivation and Deaf mental health. New York City: Routledge.
Glickman, N. (2009). Cognitive behavioral therapy for deaf and hearing persons with language and learning challenges. NYC: Routledge.
Glickman, N. (2017). Preparing deaf and hearing persons with language and learning challenges for CBT: A pre-therapy workbook.New York City: Routledge.
Gulati, S. (2014) Language deprivation syndrome. ASL Lecture Series. https://www.youtube.com/watch?v=8yy_K6VtHJw,BrownUniversity
Tobey, E.A., Geers, A.E., Sundarrajan, M. & Shin S (2011). Factors influencing speech production in elementary and high school aged cochlear implant users. Ear Hear 32 (1 Supplement): 27S-38S. doi: 10.1097/AUD.0b013e3181fa41bb
Lund, E. (2015). Vocabulary knowledge of children with cochlear implants: a meta-analysis. Journal of Deaf Studies and Deaf Education 21(2): 107-121. doi: 10.1093/deafed/env060
Pollard, R.Q. Jr., Sutter, E., & Cerulli, C. (2014). Intimate partner violence reported by two samples of deaf adults via computerized American Sign Language survey. Journal of Interpersonal Violence 29(5): 948-965. doi:10.1177/0886260513505703
Stevenson, J., McCann, D., Watkin, P., Worsfold, S., & Kennedy, C. (2010). Hearing Outcomes Study: The relationship between language development and behavior problems in children with hearing loss. Journal of Child Psychology and Psychiatry 51(1): 77-83.
Barker, D.H., Quittner, A.L., Fink, N.E., Eisenberg, L.S., TObey, E.A., & Niparko, J.K. (2009). Team CDI: Predicting behavior problems in deaf and hearing children: the influences of language, attention, and parent-child communication. Developmental Psychopathology 21(2): 373-392. doi:10.1017/S0954579409000212
Niparko, J.K., Tobey, E.A., Thal, D.J., Eisenberg, L.S., Wang, N.Y., Quittner, AL., & Fink, N.E. (2010). Team CDI: Spoken language development in children following cochlear implantation. JAMA 303(5):1498-1506. doi:10.1001/jama.2010.451
Duchesne, L. Sutton, A., & Bergeron, F. (2009). Language achievement in children who received cochlear implants between 1 and 2 years of age: group trends and individual patterns. Journal of Deaf Studies and Deaf Education 14(4): 465-485. doi.10.1093/deafed/enp010

