Articles
Important issues for our Healthy Minds community

Raising children with fetal alcohol spectrum disorders (FASD) requires unconventional parenting. To discover different ways to support my son and daughter with their challenging symptoms, I stumbled upon a service dog agency that trains dogs for children and veterans. The decision to pursue a service dog for my daughter in 2013 changed our family immeasurably.

Test your knowledge with our quiz!
This brief (6 question) quiz will test your knowledge of the most common developmental disability in the United States. Answers are provided at the end of the quiz, along with resources to learn more!

When general education teachers feel overwhelmed and unprepared to support students with Individualized Education Programs (IEPs), the benefits of inclusion can be significantly undermined. To truly embrace inclusion, we must think beyond the logistics of classroom placement and actively cultivate a learning environment where the diverse needs of all learners are acknowledged, affirmed, and celebrated as essential to the vitality and health of our schools.

FASD-informed IEPs utilize brain-based approaches to understanding, supporting, and deciding upon appropriate interventions that address the unique needs of the individual. By first understanding how FASD impacts the brain’s – and the rest of the body’s – development, we can tailor the various sections of the IEP to address the student’s unique needs.

As long as we have existed, human beings have had a symbiotic relationship with microbes. They live around us, on us, and within us. And quite literally, without them we could not survive. Scientific research on how these microbes impact our development is teaching us about the benefits of connection to nature and the challenges that come with many modern activities and perceptions.

The Juvenile Mental Health Court (JMHC) is a specialized court room within the Los Angeles County juvenile delinquency system which serves youth with developmental delays and/or significant mental health needs. It is one of dozens that are spread across the United States. Each JMHC has a slightly different focus, but all are designed to prioritize rehabilitation and treatment via community-based services rather than detention.
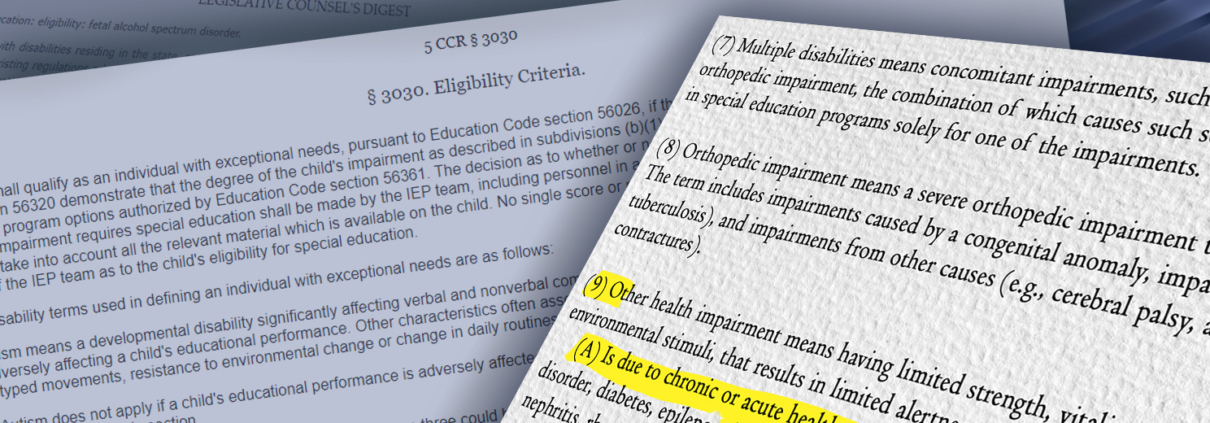
On January 1st, 2023, California’s Senate Bill 1016 became CA Education Code §56332. This law includes Fetal Alcohol Spectrum Disorders (FASD) as a named condition under the special education eligibility category of Other Health Impairment (OHI). Why is this important? And what does it mean for students, families and educators now that the law is in place?
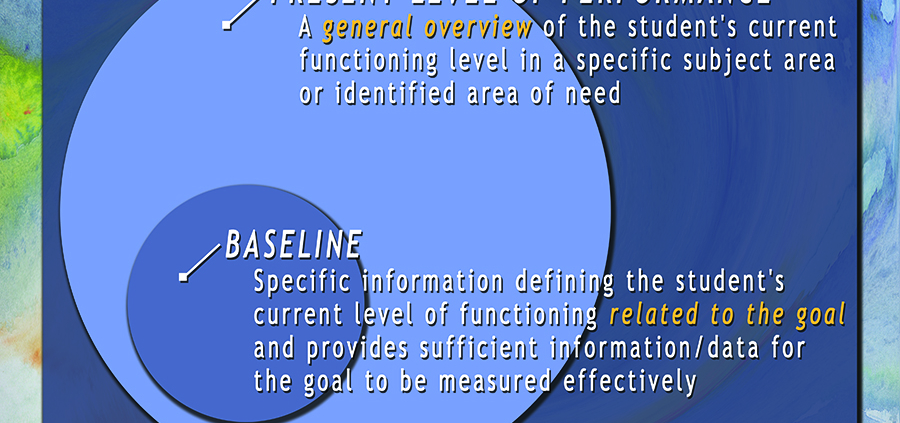
Individualized Education Programs (IEP) are both the foundation and culmination of team effort to address the needs of a student with a disability. There are many components to an IEP and seemingly as many acronyms. Many terms are used frequently but not necessarily defined meticulously and therefore some inadvertently become misused. Baseline and Present Level of Performance, for example, are often referred to interchangeably. This is understandable, as they are often closely related. There are, however, important distinctions between the two terms; they are not actually synonymous.

For centuries we have known about the impact prenatal alcohol exposure can have on a child’s development, yet the predominate culture in the United States minimizes this and turns away from acknowledgement of the repercussions. In fact, when it comes to both breadth and specificity, the known outcomes are rarely taught to professionals in the medical, educational, and mental health fields, leaving most in these disciplines ignorant of the significant needs of persons with fetal alcohol spectrum disorders (FASD).
It is time for this to change.
For Deaf and Hard of Hearing students, parents and professionals must understand that access to language and language development is a crucial part of the of the overall functioning of children and adolescents. In fact, I might argue, that understanding its impact is the central issue that school and clinical psychologists must understand in order to conduct ethical and effective evaluations of cognitive, academic and social-emotional functioning.

One of my favorite professors in college, Shoshannah Stern, is a famous Deaf actress and an incredible teacher (See: Weeds, The Hammer, Jericho). She asked us one day to consider what our reactions would be if we gave birth to a child one day who could only speak French. Well, I can only speak English. And we’re not in France, we’re in America. Would my first reaction be to learn French? Well, maybe a few key terms, but my focus would really be on trying to teach my kid English. Try to assimilate them into the culture and country in which they live. Having a deaf child is no different. That child is automatically born into a culture different than the parent, and that doesn’t happen to other families unless in very special circumstances…

In 1975, congress passed what is now commonly referred to as IDEA (Individuals with Disabilities Education Act). This act ensured that every child – no matter of ability or disability – is entitled to a free appropriate public education. In 1984, in response to major concerns that mental health services were not being adequately provided to students who needed such services in order to benefit from their education, California passed Assembly Bill 3632, which required counties to provide these services. From 1984 through 2010, the county departments of mental health were in charge of completing mental health assessments, recommendations, and case management for students. These services were coordinated with the students’ individualized education program (IEP).

There are so many complaints about how special education costs are depleting our tax dollars and diverting money that might be used elsewhere to support children’s learning. But in the view from the trenches, the expense of special education is not the culprit, inefficient spending is.
By understanding the individual and unique roles of each member of the IEP team, we can better understand and appreciate their perspective and contribution. Keeping in mind the various roles of everyone in the meeting will help in understanding where everyone is coming from and the reasons behind their positions.